[give_form id="30"]
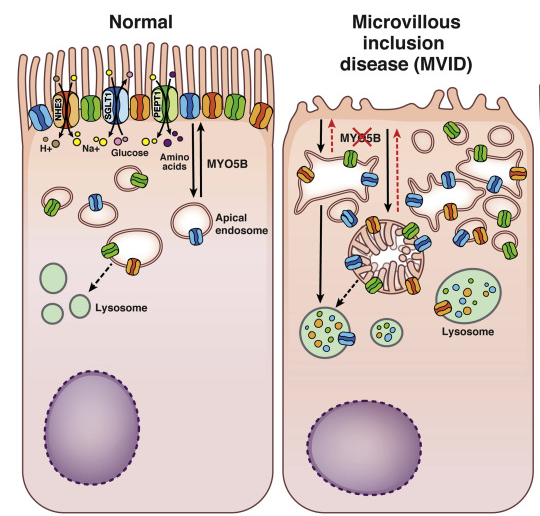
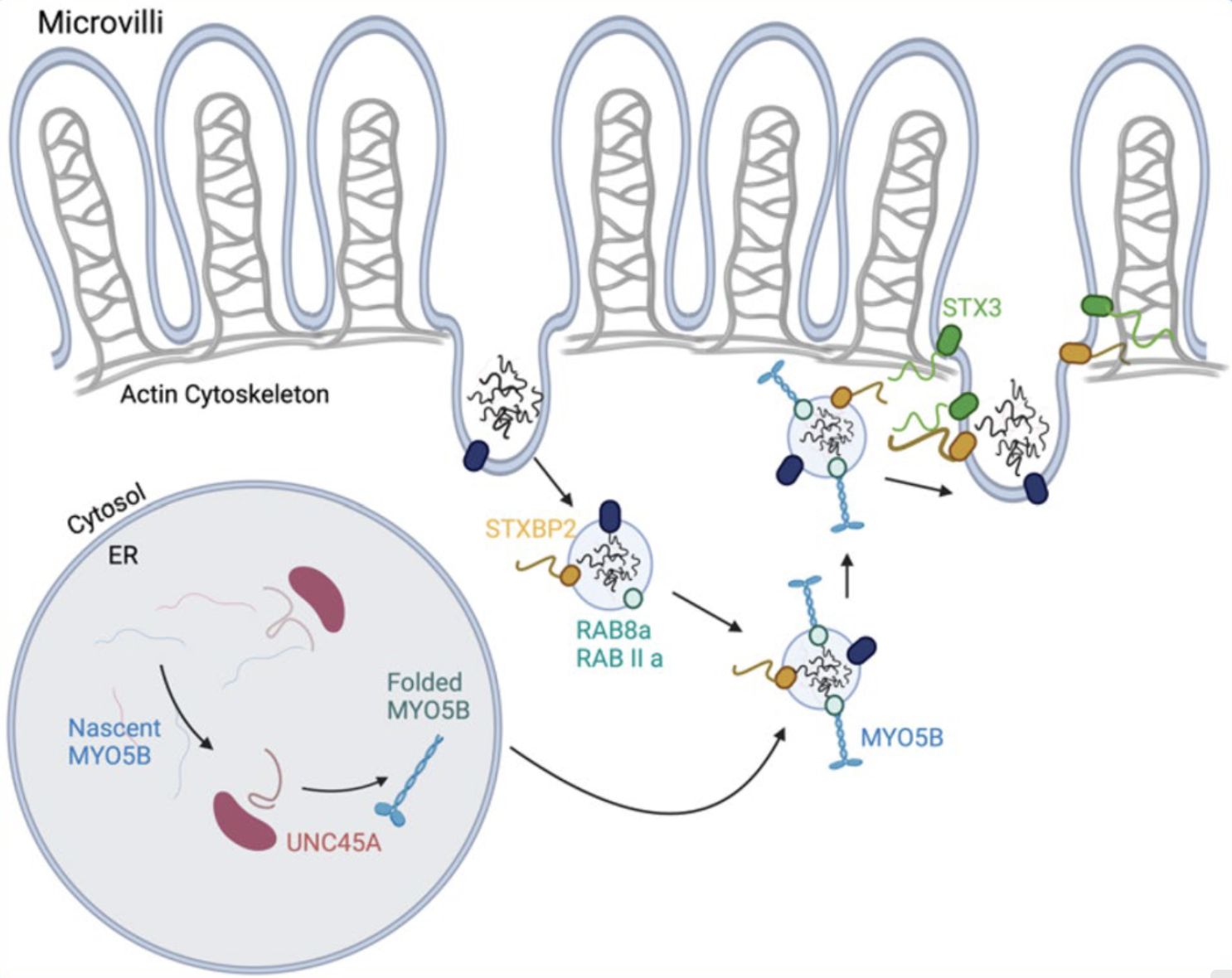
Microvillous Inclusion Disease
MVID



Affiliated Association